Categories
Change Password!
Reset Password!


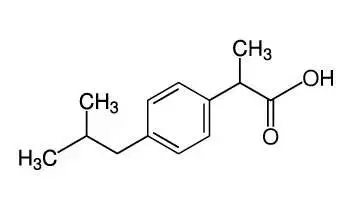
Ibuprofen, a propionic acid derivative, is a prototypical nonsteroidal anti-inflammatory agent (NSAID) with analgesic and antipyretic properties.
Ibuprofen, a propionic acid derivative, is a prototypical nonsteroidal anti-inflammatory agent (NSAID) with analgesic and antipyretic properties. Ibuprofen is indicated for the treatment of primary dysmenorrhea, osteoarthritis, rheumatoid arthritis, and for the relief of mild to moderate pain. It works by inhibition of cyclooxygenase enzyme (COX-2) which decreases the synthesis of prostaglandins involved in causing inflammation, pain, fever and swelling.
Pharmacological class: NSAID
Ibuprofen is a non-selective inhibitor of cyclooxygenase, an enzyme involved in prostaglandin synthesis via the arachidonic acid pathway. Its pharmacological effects are believed to be due inhibition of inflammatory mediators, thus acts by reducing inflammation, pain, fever and swelling. Antipyretic effects may be due to action on the hypothalamus, resulting in an increased peripheral blood flow, vasodilation, and subsequent heat dissipation. It is a racemic mixture and S-form is believed to be more pharmacologically active.
Ibuprofen is readily absorbed from GI tract (80%). Ibuprofen is a racemic mixture of R and S isomers; the R isomer (thought to be inactive) is slowly and incompletely (~60%) converted to the S isomer (active) in adults; the amount of conversion in children is not known, but it is thought to be similar to adults; a study in preterm neonates estimated the conversion to be 61% after prophylactic ibuprofen use and 86% after curative treatment (Gregoire 2004). Urine (primarily as metabolites (45% to 80%); ~1% as unchanged drug and 14% as conjugated; 1% as unchanged drug); some feces.
A study of 15 young women with primary dysmenorrhea was carried out to assess the prophylactic administration of ibuprofen for the treatment of severe and disabling primary dysmenorrhea. The study lasted for six months. The treatment schedule included 400 mg of ibuprofen every 8 hours, starting 24 hours before the menstrual cycle during 4 days of menstruation for six consecutive cycles. Results showed that the mean of initial intensity of menstrual cramp experienced in the cycle before treatment (control) was 9.47 +/- 0.5. During prophylactic treatment, the means of initial intensity of pain were significantly lower, between 7.84 +/- 0.37 and 7.21 +/- 0.52. A statistically significant progressive decrease of pain was recorded during the duration of treatment. After 48 hours of treatment, intensity of pain was recorded as three (mild). Results from study proves that prophylactic administration of ibuprofen is an effective treatment for selected women experiencing severe and disabling primary dysmenorrhea.1













Comments (0)