Categories
Change Password!
Reset Password!


Bismuth quadruple therapy is useful to treat H. pylori infections that have 23S rRNA point mutations.
In a randomized controlled study, concomitant therapy (CoT) and tailored therapy (TaT) exhibited comparable overall elimination rates for Helicobacter pylori (H. pylori). But, CoT elimination rate was suboptimal, particularly in point mutation-positive people. In individuals having point mutations in 23S rRNA gene, Su Jin Kim et al. compared the rate of eradication of the empirical CoT and tailored therapy TaT utilizing Bismuth quadruple therapy (BQT) rather than PPI, Amoxicillin, Metronidazole (PAM).
A total of 290 people were recruited and were split into 2 groups at random. For 14 days, patients in the CoT group got twice daily doses of 500 mg Metronidazole, 500 mg Clarithromycin, 1 g Amoxicillin, and 20 mg Rabeprazole. Patients in the TaT group who tested negative for point mutations got 500 mg Clarithromycin, 1 g Amoxicillin, and 20 mg Rabeprazole two times a day for 14 days, while those who tested positive for point mutations received 20 mg Rabeprazole twice daily, 500 mg Metronidazole 3 times a day, and 120 mg Bismuth and 500 mg Tetracycline 4 times a day for 14 days.
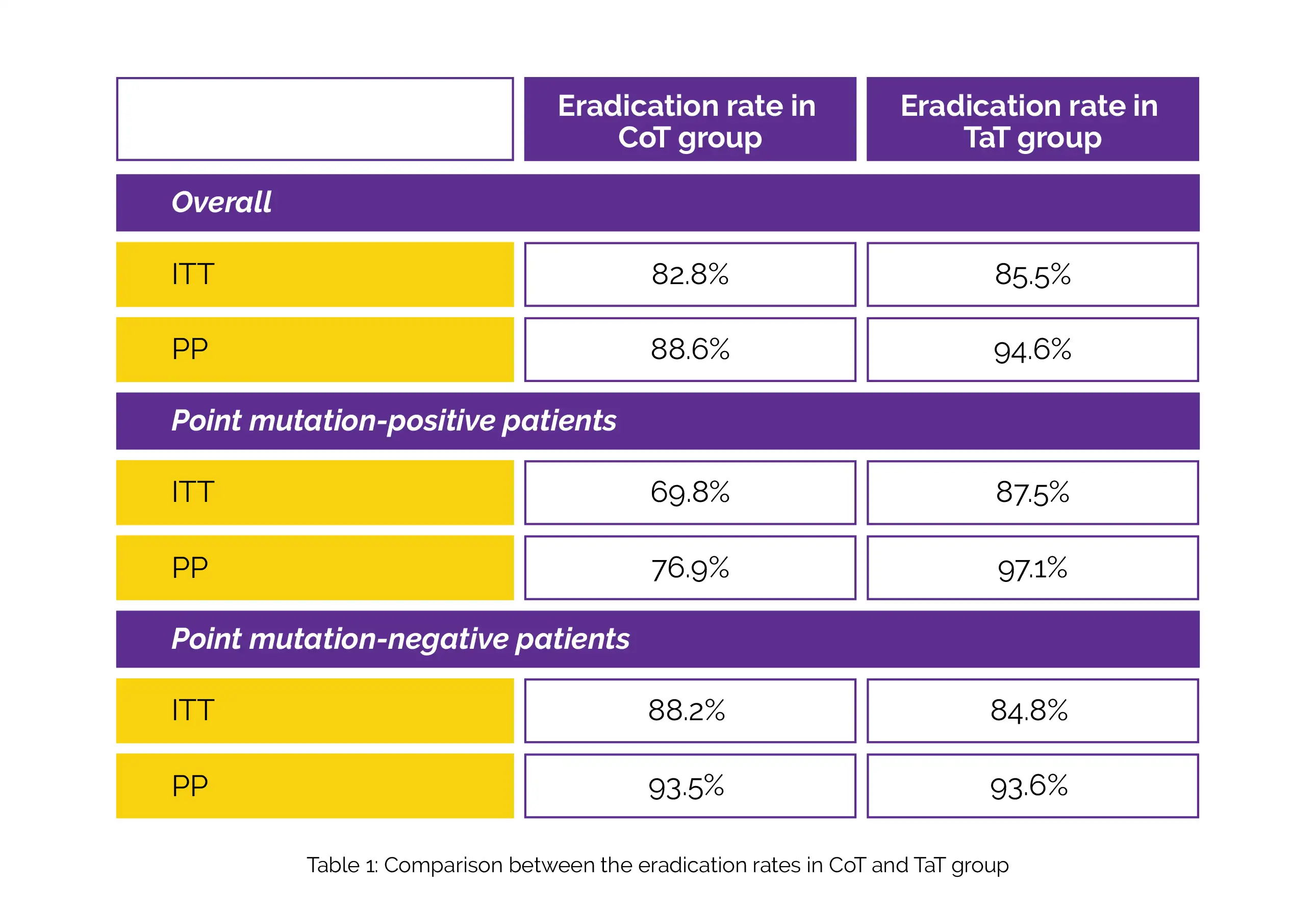
Intention-to-treat (ITT) and per-protocol (PP) studies each included 290 and 261 patients, respectively. In 28.6% of the patients, A2142G and/or A2143G point mutations were found. According to analyses conducted using ITT and PP, there was no discernible difference in the overall eradication rates between the 2 groups. According to ITT and PP assessments, the rate of elimination in the CoT group was lower than those in the TaT group in subjects who tested positive for point mutations. On the other hand, there was no considerable difference in the elimination rates who tested negative for point mutations, as shown in Table 1:
For H. pylori-infected individuals harboring 23S rRNA point mutations and who have developed Clarithromycin resistance, BQT is beneficial as the first line of therapy.
Medicine (Baltimore)
A randomized controlled trial to compare Helicobacter pylori eradication rates between the empirical concomitant therapy and tailored therapy based on 23S rRNA point mutations
Su Jin Kim et al.














Comments (0)